

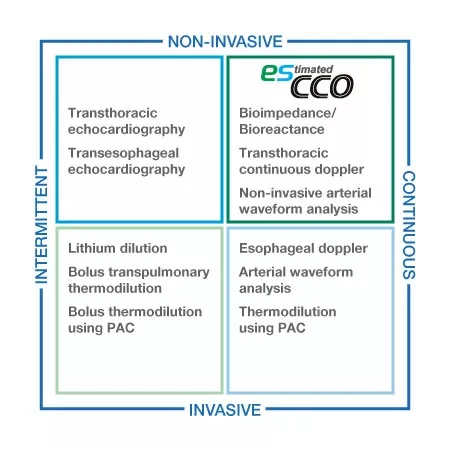
esCCO
The next generation of non-invasive hemodynamics monitoring
esCCO 와 함께 진료의 질 재정의
Nihon Kohden은 침습 정도와 관계없이 모든 치료 환경에 혈류량 정보를 제공하는 혁신적인 기술인 esCCO(추정 연속 심박출량)를 통해 의료 서비스의 질을 새롭게 정의하고 있습니다.
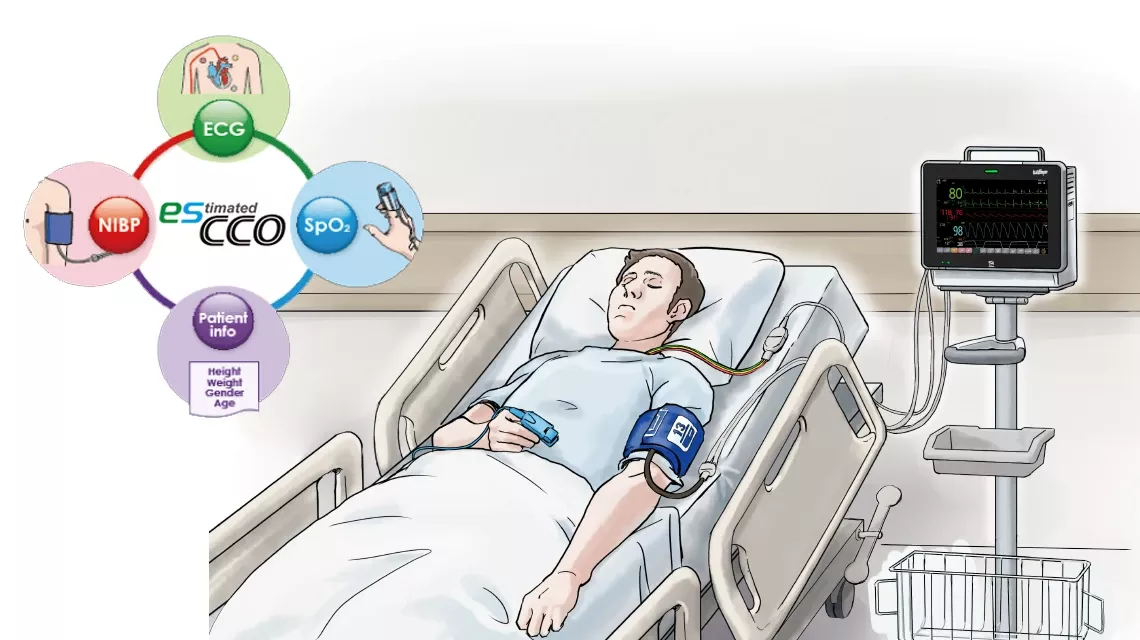
esCCO는 맥파 전달 시간(PWTT)을 이용하여 심박출량(CO)을 산출하는 새로운 기술로, 맥박산소측정기와 심전도(ECG) 신호를 활용합니다..
심박출량(CO) 및 일회박출량(SV)의 변화를 추적하는 esCCO의 추세 추적 성능은 임상 연구를 통해 평가되었으며, 그 정확성 또한 임상적으로 활용 가능한 수준임이 입증되었습니다.1, 2
이를 통해 비용 문제나 인력 부족으로 인해 CO 측정이 어려웠던 환자들에게도 최적의 혈역학적 관리를 제공할 수 있습니다.
신뢰할 수 있는 추세 성과
천만히
추가 센서는 없습니다
체액 관리 최적화를 위한 esCCO
박출량과 심장 지수와 같은 부피 지표를 기반으로 한 최적의 수액 관리가 환자 개선에 도움이 될 수 있다는 보고가 있습니다 3, 4 결과로는 입원 기간이 단축되고 합병증이 감소하는 것이 포함됩니다 . 따라서 이제 더 나은 환자 치료를 위해 혈역학적 경향을 관리하는 침습이 적고 효율적인 방법에 대한 수요가 증가하고 있습니다 . 비침습적이고 사용하기 쉬운 esCCO 는 현재 시장에 나와 있는 다른 방법들의 단점을 보완하여 이 목적에 유용한 솔루션을 제공할 수 있습니다 .
모든 케어 수준에 대한 체적 정보
모든 케어 수준에 대한 체적 정보 esCCO 는 심전도 , SpO2, 혈압 등 일반적인 활력 징후 지표만을 사용하여 심박출량 정보를 제공하며, 추가 센서나 특별한 훈련이 필요하지 않습니다. esCCO 는 주요 수술뿐만 아니라 출혈이나 혈역학적 스트레스 가능성이 높은 고위험 환자의 저위험 시술에서도 모든 치료 수준에서 혈역학적 추세 모니터링을 제공합니다. 또한 esCCO 는 다양한 임상 환경에서 수액 투여 시 신뢰할 만한 지표가 될 수 있습니다. 기존 환자 모니터링에 esCCO 를 추가하면 수액 관리 최적화, 합병증 위험 감소, 궁극적으로는 입원 기간 단축 등 더 나은 결과를 얻을 수 있습니다.
esCCO 의 잠재적 응용
폐동맥 또는 경폐 열희석 카테터 제거 후 혈류역학 모니터링.
더 공격적이고 위험한 기법 ( 예 : 폐동맥 카테터 ) 을 사용할 수 없는 환자의 혈역학적 최적화
목표 지향적 유동적 관리 등 의사결정 과정 지원.
갑작스러운 악화를 조기에 감지하기 위한 분류 도구 .
1 Ishihara H, Okawa H, Tanabe K, Tsubo T, Sugo Y, Akiyama T, Takeda S. A New Non-Invasive Continuous Cardiac Output Trend Solely Utilizing Routine Cardiovascular Monitors. J Clin Monit Comput 2004; 18: 313–320.
2 Yamada T, Tsutsui M, Sugo Y, Sato T, Akazawa T, Sato N, Yamashita K, Ishihara H, Takeda J. Multicenter Study Verifying a Method of Noninvasive Continuous Cardiac Output Measurement Using Pulse Wave Transit Time: A Comparison with Intermittent Bolus Thermodilution Cardiac Output. Anesth Analg. 2012 Mar 30
3 Wakeling HG et al. Intraoperative oesophageal Doppler guided fluid management shortens postoperative hospital stay after major bowel surgery. Br J Anaesth 2005; 95 : 634-42.
4 Mayer J et al. Goal-directed intraoperative therapy based on autocalibrated arterial pressure waveform analysis reduces hospital stay in high-risk surgical patients: a randomized, controlled trial. Crit Care 2010; 14: R18.
esCCO의 원리
esCCO의 핵심 기술인 맥파 전달 시간 (Pulse Wave Transit Time, PWTT)
맥파 전달 시간 (Pulse Wave Transit Time, PWTT) 은 심전도(ECG)의 R파 피크 시점부터 맥파 상승점 (pulse wave rise point) 까지의 시간으로 정의됩니다. 맥파 상승점은 미분된 맥파 (differentiated pulse wave) 가 최대 진폭의 30%에 도달하는 지점으로 정의됩니다¹. PWTT는 세 개의 구간으로 구성됩니다. 즉, 전박출기 (Pre-Ejection Period, PEP), 탄성 동맥(elastic artery)을 통한 맥파 전달 시간 (T1), 그리고 말초 동맥 (peripheral arteries)을 통한 맥파 전달 시간 (T2) 입니다 (Figure 1).
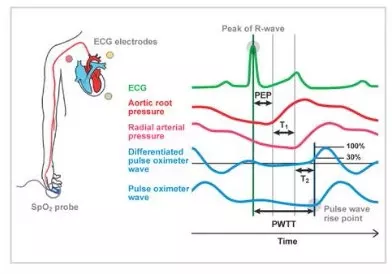
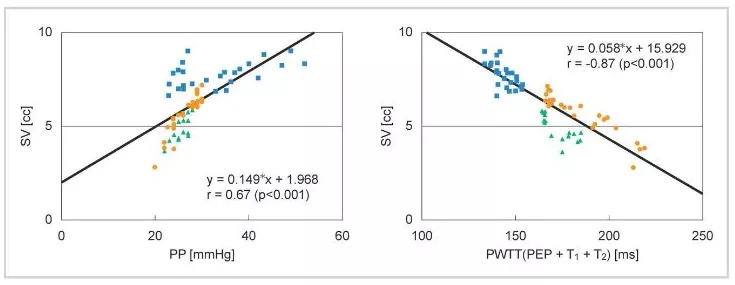
PEP는 심장 수축력 (cardiac contractility) 과 전부하 (preload) 를 반영하며, 심장 수축력과 전부하가 증가할수록 짧아집니다. T1은 동맥 순응도 (arterial compliance) 에 의존하며, 혈압이 상승하면 짧아집니다. T2는 혈관이 확장될 때의 혈관 저항 (vascular resistance) 을 반영합니다. 이처럼 PWTT에는 혈역학적 관리 (hemodynamic management) 와 관련된 다양한 요소가 포함되어 있으며, 여기에 심박출량 (CO) 과 관련된 생리학적 소견을 결합하여 임상 적용 가능성을 검증해 왔습니다. 그 결과, 초기에는 PWTT를 이용하여 혈압을 추정하려는 시도가 이루어졌습니다. 그러나 심혈관 작용제 (cardiovascular agonist drugs) 를 투여했을 때 PWTT의 변화 양상이 달라진다는 사실이 확인되었습니다. 또한 약물 투여 시 혈압 변화와 일회박출량 (SV) 의 변화가 일치하지 않는 경우에도, PWTT와 일회박출량 (SV) 은 우수한 상관관계를 보이는 것으로 관찰되었습니다 (Figure 2).
esCCO 계산식
기존의 심박출량 측정 장치는 동맥 혈압 파형에서 출력을 계산하는 펄스 윤곽법을 측정 원리로 사용합니다. 이는 박수량(SV)과 맥박압(PP) 사이에 좋은 상관관계가 있음을 보여줍니다 (식(1)).
SV = K × PP (1) K: a constant
또한 esCCO의 기본 개념에서 그림 2의 PWTT와 SV는 좋은 상관관계를 가지며, 이는 식(2)으로 나타날 수 있습니다.
SV = α’ × PWTT + β’ (2) α’: a constant β’: a coefficient
식(2)은 방정식 (1)을 사용하여 준수 성분 K를 포함함으로써 식(3)으로 확장할 수 있습니다.
SV= K × ( α × PWTT + β ) (3) α: a constant, β and K: coefficients
위에 따르면, 심박출량은 PWTT를 사용해 연속적으로 측정되며, esCCO는 식(4)을 사용해 얻어집니다.
CO = SV × HR = K × (α × PWTT + β) × HR = esCCO (4)
α: a constant, β and K: coefficients
esCCO 보정
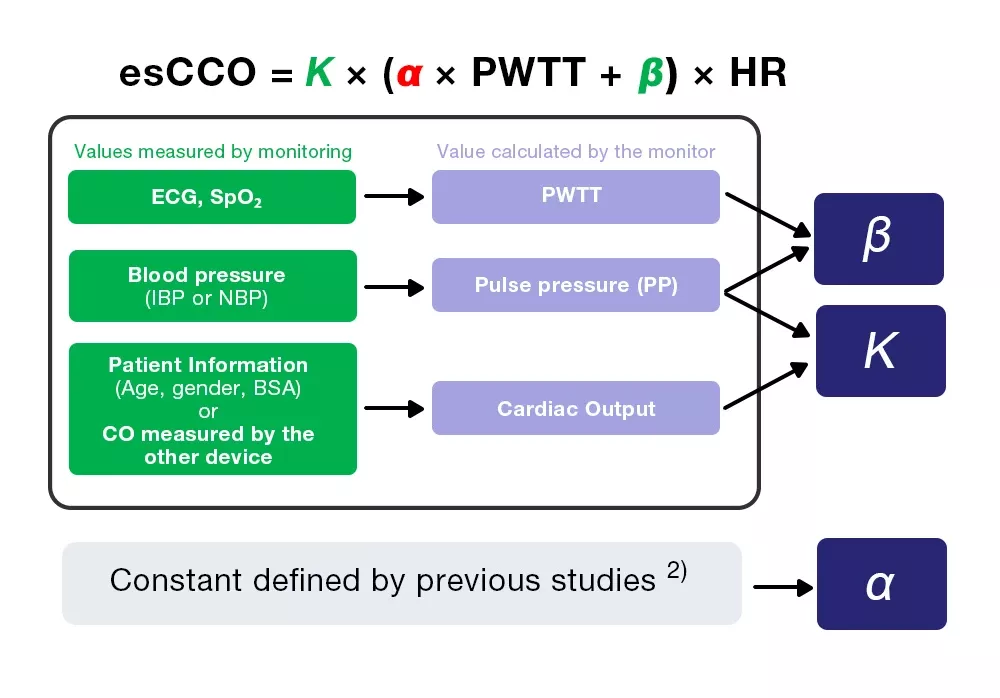
esCCO는 세 가지 계수(K, α, β)를 포함하는 식(4)에서 심박출량을 얻습니다.
esCCO = K × (α ×PWTT +β) ×HR (4)
세 계수 중 α는 이전 연구에서 얻은 상수(2)이다. K와 β는 보정 중 모니터링으로 계산된 세 가지 값(PWTT, PP, CO)을 입력하여 결정됩니다.
하지만 교정을 위한 CO는 환자 정보에서 얻어져 비침습적 측정이 가능하며, 이는 esCCO의 가장 큰 특징 중 하나입니다.
Reference
1) Sugo Y, UkawaT, Takeda S, Ishihara H, Kazama T, Takeda J. 2010. A Novel ContinuousCardiac Output Monitor Based on Pulse Wave Transit Time. Conf Proc IEEE Eng MedBiol Soc. 2010: 2853-6.
2) Ishihara H, Okawa H, Tanabe K, Tsubo T, Sugo Y, Akiyama T, Takeda S. A New Non-Invasive Continuous Cardiac Output Trend Solely Utilizing Routine Cardiovascular Monitors. J Clin Monit, 2004; 18: 313–320.
근거 기반 수행
2004년에 우리는 esCCO가 연속심박출량(CCO)과 높은 상관관계를 보인다고 보고했습니다.
여러 임상 검사를 수행하면서, 정확도와 반응성에 관한 다음 보고서가 작성되었으며, 이는 측정 성과의 핵심 포인트입니다.
측정 정확도
2009년에는 esCCO의 실용적 적용 효과가 일본 내 7개 시설에서 다기관 연구에서 평가되었으며, 연구 결과는 2012년에 논문으로 보고되었습니다.
Multicenter Study Verifying a Method of Noninvasive Continuous Cardiac Output Measurement Using Pulse Wave Transit Time: A Comparison with Intermittent Bolus Thermodilution Cardiac Output
Authors: Yamada T, Tsutsui M, Sugo Y, Sato T, Akazawa T, Sato N, Yamashita K, Ishihara H, Takeda J. Reference: Anesth Analg 2012;115:82-6. July 2012, Vol.115, No.1.
Background
덜 침습적인 심박출량 모니터링을 위한 많은 기술이 개발되었습니다. esCCO는 PWTT를 이용해 심박출량을 측정하는 기술 중 하나입니다. 심전도, SpO2, 혈압의 기본 모니터링과 함께 ECG 전극, SpO2 프로브, 커프를 이용한 경우, esCCO는 저위험 환자를 포함한 모든 환자의 임상 순환 모니터링에 적용될 수 있습니다. esCCO의 효능은 PWTT를 사용하여 다기관 공동 연구에서 평가되었습니다.
Method
연구는 일본 7개 시설에서 213건 (중환자실 139건, 수술실 74건) 에서 간헐적 볼루스 열희석 (ICO) 으로 측정한 esCCO와 심박출량을 비교했습니다. 모든 환자에 대해 심전도 (ECG), SpO2 및 침습적 혈압을 측정했으며, esCCO는 한 번 보정되었습니다. ICO 측정을 위해 ICU 환자는 하루 한 번, 수술실 환자에게는 시간별로 심박출량을 측정했으며, ICU 및 수술실 환자 모두 폐동맥 카테터 제거 직전에 측정했습니다. ICO와 esCCO는 상관분석과 Bland-Altman 분석을 통해 비교되었으며, 시간에 따른 편향 변화도 평가하였다.
Result
esCCO와 ICO 간의 상관관계 총 213명의 환자로부터 587개의 측정 지점이 얻어졌습니다. 환자 인구 통계는 표 1에 나와 있습니다.
| n | Age | Gender (M/F) | Height (cm) | Weight (kg) | BSA (㎡) | |
|---|---|---|---|---|---|---|
| Total | 213 | 65.1 ± 12.7 | 142/71 | 160.0 ±10.3 | 59.2 ±12.5 | 1.61 ±0.20 |
Table 1. Patient demographics
esCCO와 ICO 간의 상관관계는 다음과 같았습니다 r = 0.79 (p<0.01) and bias ± precision was 0.13 ± 1.15 (L/min), 이는 esCCO가 ICO와 동등한 우수한 측정 정확도를 가진다는 것을 시사합니다 (Figure 4).
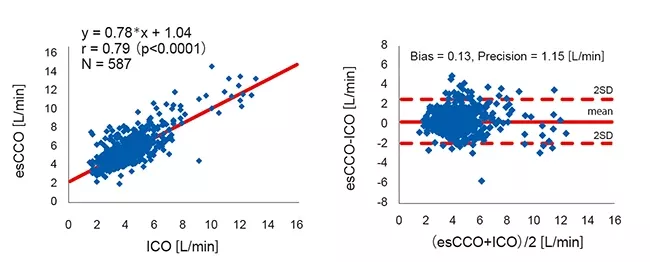
esCCO와 ICO 간 평균 편향에 대한 95% 신뢰구간은 0.04에서 0.22였습니다. 이는 임상적으로 허용되는 범위 ±0.3(L/min) 범위 내에 있었습니다3.
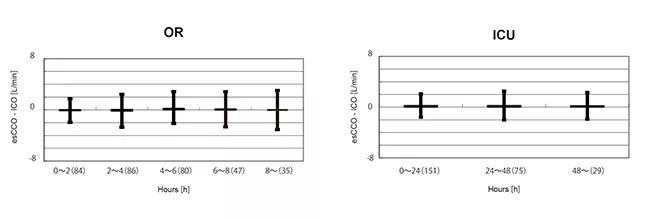
T시간에 따른 편향 변화를 평가하기 위해, OR 그룹에서 교정 후 기간의 데이터를 2시간씩 5개의 구간으로 나누었습니다. 이 5개 구간의 편향에서는 유의미한 차이가 발견되지 않았습니다. (Welch's ANOVA p = 0.07)
또한 ICU 그룹에서는 교정 후 데이터가 24시간씩 3개의 간격으로 나뉘었습니다. 이 세 구간의 편향에는 유의미한 차이가 발견되지 않았습니다. (Repeated-measures ANOVA P = 0.781) (Figure 5).
Summary
esCCO와 ICO 사이에는 강한 상관관계가 있었고 편향은 작았습니다. 시간에 따른 편향 변화도 작았습니다.
반응성
2015년에는 침습적 혈압 파형(APCO)을 기반으로 한 측정 방법과의 비교가 보고되었으며, 이 방법은 많은 시설에서 심박출량을 측정하는 데 널리 사용됩니다.
간헐적 볼루스 열희석(ICO)에 의한 심박출량을 비교의 기초로 사용했으며, 시간에 따른 변화 비교 결과 반응성이 APCO와 유사함을 확인하였습니다.
Comparison of the ability of two continuous cardiac output monitors to measure trends in cardiac output: estimated continuous cardiac output measured by modified pulse wave transit time and an arterial pulse contour-based cardiac output device
Authors: Terada T, Oiwa A, Maemura Y, Robert S, Kessoku S, Ochiai R.Reference: J Clin Monit Comput. 2015 Sep 14.
Background
신장 이식은 심박출량 증가와 동맥압 및 혈관 저항 감소를 동반하는 다양한 심혈관 이상과 관련이 있습니다. 따라서 이러한 지표의 수술 전후 모니터링은 신장 이식 환자에게 매우 중요합니다.
T본 연구는 esCCO(간헐적 볼루스 열희석(ICO)로 측정된 심박출량과 동맥 혈압 파형 관찰을 기반으로 한 심박출량(APCO)을 비교하였습니다.
Method
신장 이식이 예정되어 있고 동의를 제공할 수 있는 성인 환자들이 도호 대학 오모리 의료센터에서 평가에 등록되었습니다.
모든 환자에서 ECG, SpO2 및 침습적 혈압을 측정하였습니다.
ICO, esCCO 및 APCO는 마취 유도 후, 이식 신장 봉합 시작 전, 동맥 압박(동맥 재혈관화) 전, 그리고 수술 종료 시 4회 측정되었습니다.
각 알고리즘의 결과는 상관분석, 블랜드 및 알트만 분석, 극지방 플롯 분석을 통해 비교되었습니다.
Result
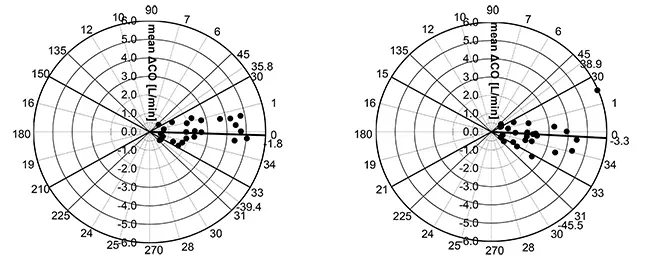
esCCO와 ICO의 평균 각도 편향은 -1.8°였고, 일치의 반경 한계는 37.6°. (Figure 6. Left)
APCO와 ICO의 평균 각도 바이어스는 -3.3°였으며, 반경 일치 한계는 42.2°± 되었습니다. (Figure 6. Right).
따라서 esCCO와 ICO 간의 상관관계, 편향, 추세 능력은 APCO와 ICO 간의 상관관계, 편향, 추세 능력과 유사하다고 말할 수 있습니다.
사례 보고서(Figure 7)는 esCCO의 추세 능력이 APCO와 비교할 만함을 보여줍니다.
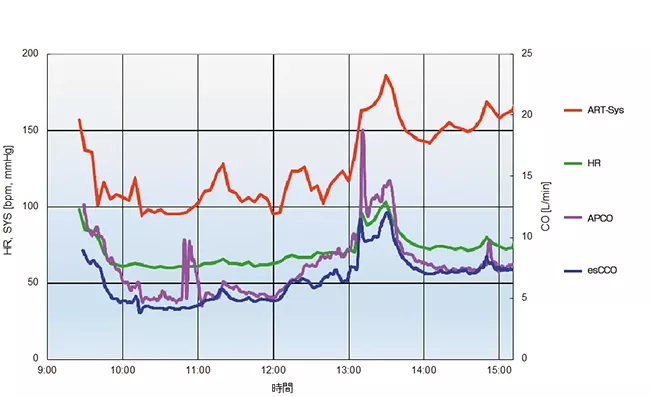
31세 남성, 키 180cm, 몸무게 93.8kg. 측정된 APCO와 esCCO의 측정값은 각각 마취 유도 후 6.5 L/min과 4.7 L/min, 이식 신장 봉합 시작 전 7.3 L/min과 6.5 L/min, 수액 채취 후 동맥 클램프(artery reperfusion) 전 14.3 L/min과 12.0 L/min, 그리고 수술 종료 시 7.4 L/min과 7.4 L/min이었습니다.
Summary
esCCO의 추세 추적 능력은 임상적으로 수용 가능하며 동맥압 파형 분석법과 동등한 수준이다.
Reference
1) Ishihara et al. 2004. A new non-invasive continuous cardiac output trend solely utilizing routine cardiovascular monitors. J Clin Monit, Dec, 18: 313-320.
2) Lawrence C. Siegel, Maeve M. Hennessy, Ronald G. Pearl. 1996. Delayed Time Response of the Continuous Cardiac Output Pulmonary Artery Catheter. Anesth Analg
FAQ
esCCO는 심박출량을 지속적이고 비침습적으로 측정하는 새로운 기술입니다. 이 페이지는 가장 자주 받는 질문들을 위한 FAQ 페이지입니다.
어린이와 신생아도 측정할 수 있나요?
네, 하지만 임상 근거가 없어서 권장하지는 않습니다.
- esCCO 측정은 신생아에서 검증되지 않았습니다. 신생아의 혈관 특성은 일반적으로 성체와 다르기 때문에 파동 전파 특성에 영향을 받습니다.
- 어린이의 경우, 환자 정보를 이용한 CO 교정 시 회귀방정식 결정 시 소아 데이터가 포함되지 않아 esCCO 값이 과대평가될 수 있습니다.
맥박 산소 측정기 프로브를 발가락이나 귀에 부착할 수 있나요?
네, 하지만 임상적 근거가 없기 때문에 권장되지는 않습니다.
PWTT는 혈관 길이와 그 순응성에 따라 달라지므로, 부착 부위에 따라 달라질 수 있습니다. 현재 esCCO는 주로 손가락을 기준으로 평가되며, 발가락이나 귀에 대한 검증은 이루어지지 않았습니다.
esCCO 측정 중 프로브 부착 부위가 손가락에서 발가락, 귀로 바뀌면 PWTT가 변하고 esCCO 값이 크게 변할 수 있으므로 주의하세요.
캘리브레이션은 언제 해야 하나요? 교정 작업은 언제 수행해야 하나요?
마취 유도 후 교정이 권장됩니다.
esCCO의 효과 평가는 주로 마취 유도 후 시작된 침습적 CO 측정과 비교하여 확인되었습니다.
마취 유도 전 환자는 긴장하고 혈압이 높으며 심박수가 빨라서 보정 시 esCCO 값이 과도하게 나타나는 경향이 있습니다.
또한, 마취 유도 시 호흡과 신체 움직임에 따라 프로브가 움직이기 때문에 펄스파의 안정적 탐지가 어려워지고 보정이 어려울 수 있습니다.
마취 유도 후 혈압과 심박수가 비교적 안정적이어서 PWTT가 안정되어 보정이 더 쉬워졌습니다.
재조정은 언제 필요한가?
예를 들어, 보정 시점과 PWTT의 상관관계가 크게 변하는 경우, 예를 들어 esCCO 값이 유의미하게 변할 경우 재보정을 권장합니다.
심전도: 유도 심전도 변화, QRS 형태가 크게 변함.
기타: 심박수 및 맥박파 센서의 부착 부위가 환자의 신체 자세(얼굴을 위로 한 자세에서 측면 위치로)의 변화나 심폐 우회술(CPB) 또는 심장 판막 교체 후 변경되는 경우.
esCCO가 적용되지 않는 경우는 언제인가요?
다음 상황과 사례는 적용되지 않는 것으로 간주됩니다.
심장 수술: esCCO는 PWTT를 기반으로 심박출량을 측정합니다. 병든 심장에서는 안정적인 PWTT를 얻지 못하거나, 심장이나 대혈관계에 가해지는 스트레스로 인해 PWTT를 측정할 수 없는 상황이 발생할 수 있습니다.
전기소작이 자주 사용되는 경우: 전기소작 소음이 심전도에 영향을 미쳐 PWTT 측정이 불가능해집니다.
페이싱이 허용되지 않는 등 다른 제한 사항들은 운영 매뉴얼에 명시되어 있습니다.
자료 다운로드―esCCO
Learn more

Experience with esCCO in Surgery in Elderly Patients

Hemodynamic Management Using esCCO

Hemodynamic Evaluation Using esCCO during Cesarean Section under Spinal Anesthesia

Can Estimated Continuous Cardiac Output Be Used in the Same Manner as Arterial Pressure-Based Cardiac Output?

Continuous Cardiac Output from ECG and SpO2

Non-Invasive Hemodynamics Monitoring

Improving the standard of non-invasive hemodynamic monitoring

Hemodynamics Graph for GDT

Hemodynamic Management Using Estimated Cardiac Output (esCCO)

Anesthesia Management Using Estimated Continuous Cardiac Output (esCCO)

Comparison of trend performance of esCCO and APCO in kidney transplantation

esCCO Performance Report